

INTRODUCTION
Acute Graft-versus-host disease (aGVHD) is a common complication of allogeneic hematopoietic cell transplantation (HCT), affecting about 50% of transplants. Grading of aGVHD can serve a variety of purposes, including retrospective assessment of peak severity, real-time assessment of severity at prespecified time points, and determination of the need for treatment. But several problems hamper the application of grading systems to predict outcomes among patients with aGVHD: (1) Assignment of a peak GVHD score is done retrospectively; clinicians cannot use the current grading system for peak score in real-time1. (2) The systems do not account for the time to the response after treatment1. (3) Assignment of grade IV GVHD is often used to indicate that GVHD caused a death, irrespective of the severity. In this situation, the grading reflects the outcome and cannot be used to predict the outcome1.
Recently serum biomarkers have emerged as an additional potential measurement of acute GVHD severity. The Mount Sinai Acute GVHD International Consortium (MAGIC) Group, has validated MAGIC algorithm probability (MAP) that combines two GI biomarkers (ST2 and REG3α) into a single value. The MAP predicts response to treatment, GVHD severity. But in resource-limited settings, like transplant centers in India lack testing features.
In this study we have developed a risk scoring based on clinical and easily available biochemical parameters to predict the severity of aGVHD.
AIMS AND OBJECTIVES
To predict the aGVHD severity at the onset based on risk factor score.
To assess the steroid response in different risk groups
MATERIAL AND METHODS
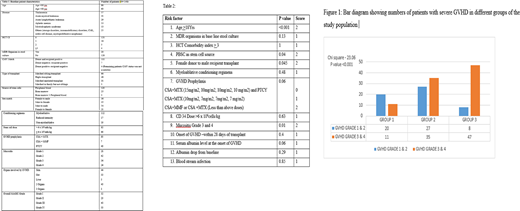
The study included patients who underwent allogeneic HCT at Narayana hrudayalaya hospital, between January 2015 and April 2020 and developed acute GVHD within 100 days of transplant. After taking institutional ethics committee approval, data were collected from medical records. Baseline patient characteristics are mentioned in table 1. The following parameters were analyzed as risk factors for the development of severe GVHD (MAGIC grade 3 and 4): 1. Age >18 yrs, 2. MDR organisms in baseline stool culture, 3. HCT comorbidity index >1, 4. Peripheral blood as a source of stem cells, 5. Female to male transplants, 6. Myeloablative regimens, 7. Suboptimal GVHD prophylaxis, 8. CD34 dose > 6 x 106/kg, 9. Grade 3/4 mucositis 10. Early-onset GVHD (within 28 days), 11. Albumin level at the onset of GVHD, 12. Albumin drop from baseline3, and 13. Bloodstream infection. Risk factors with a p-value of <0.05, were given score 2 and score 1 was given to other parameters. The total score ranged from 0 to 17. The study population was divided into 3 groups (Group 1 with score 0-4, Group 2 with score 5-7, Group 3 with score > 8). The following outcomes were assessed in each group; severity of GVHD (Grade I/II vs Grade III/IV) and response to steroids.
RESULTS
Out of 148 patients, 35.5% of Group 1, 56.5% of Group 2 patients and 85.5% of Group 3 patients developed Grade 3 or 4 GVHD respectively (P-value <0.001). Positive predictive value of score > 8 to predict Grade 3/4 GVHD is 85.4%, negative predictive value is 50.6%, sensitivity is 50.5%, and specificity is 85.5%. From Group 1 and 2, only 30% of patients were steroid non responders, while 55.3% of Group 3 patients are steroid non responders (P-value - 0.04).
CONCLUSION
Traditional GVHD scoring systems reflect the outcome and cannot be used to predict the outcome. Various biomarker-based scoring systems are helpful in this situation, but in resource-limited settings, it might not be easily feasible. Clinical scoring systems like risk factor-based scoring systems are very helpful, which can predict the severe GVHD at early time points leading to management decisions such as upfront initiation of aggressive treatments and earlier introduction of second-line agents.
References
Leisenring WM, et al. An acute graft-versus-host disease activity index to predict survival after hematopoietic cell transplantation with myeloablative conditioning regimens. Blood. 2006;108(2):749-55.
2.Rashidi A, et al. Peritransplant Serum Albumin Decline Predicts Subsequent Severe Acute Graft-versus-Host Disease after Mucotoxic Myeloablative Conditioning. Biol Blood Marrow Transplant. 2016;22(6):1137-41.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal